
Snake Arenavirus (Reptarenavirus, IBD): Virology, Pathogenesis, and Diagnostics
Introduction
Inclusion body disease (IBD) is a highly significant and frequently fatal viral syndrome affecting captive boid and pythonid snakes worldwide. For decades, the etiological agent of IBD remained elusive, with various hypotheses proposed. Definitive identification of the causative agent was achieved through metagenomic sequencing and viral isolation, which revealed a novel group of arenaviruses, now classified within the genus Reptarenavirus (family Arenaviridae) [1]. This discovery fundamentally reshaped the understanding of IBD, transitioning it from a histopathological diagnosis to a molecularly defined viral disease. This article provides a detailed veterinary reference on snake arenaviruses, covering their taxonomy, virion structure, genomic organization, replication cycle, pathogenesis, clinical presentation, diagnostic approaches, and management strategies.
Taxonomy and Classification
Snake arenaviruses are classified within the family Arenaviridae, a diverse family of enveloped, single-stranded RNA viruses. The family Arenaviridae is divided into several genera, including Mammarenavirus (which includes many human pathogens such as Lassa virus and lymphocytic choriomeningitis virus), Reptarenavirus, Hartmanivirus, and others. The genus Reptarenavirus was established to accommodate the arenaviruses identified in snakes [1]. The type species is Reptarenavirus boidae, with the Golden Gate virus (GGV) serving as the prototype strain. Other reptarenaviruses, such as the University of Giessen virus (UGV) and the California Academy of Sciences virus (CASV), have also been characterized [1]. These viruses are genetically distinct from mammalian arenaviruses, exhibiting significant divergence in their nucleoprotein (NP) and glycoprotein (GP) sequences [1].
Virion Structure and Genomic Organization
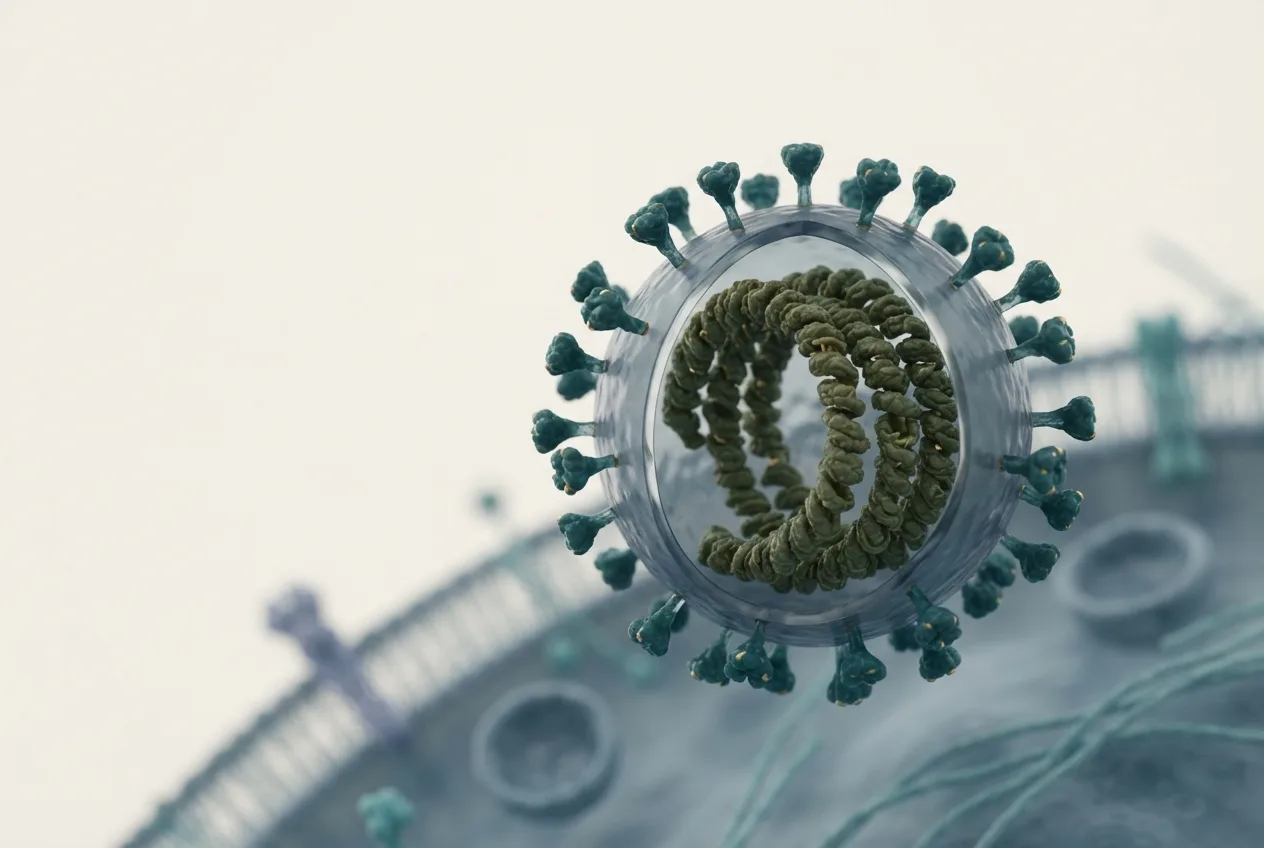
Reptarenavirus virions are pleomorphic, spherical to oval particles, typically 80 to 150 nm in diameter, as observed by electron microscopy [1]. They are enveloped, with the lipid envelope derived from the host cell plasma membrane. The envelope is studded with glycoprotein spikes, which are essential for host cell attachment and entry.
The genome consists of two single-stranded, negative-sense RNA segments, designated L (large) and S (small) [1]. This bipartite genome organization is characteristic of the Arenaviridae family.
Genomic Segment Characteristics:
| Segment | Length (approximate) | Encoded Proteins | Function | | :-, | :-, | :-, | :-, | | L segment | ~7.2 kb | RNA-dependent RNA polymerase (L protein) | Viral genome replication and transcription | | S segment | ~3.5 kb | Nucleoprotein (NP) and Glycoprotein precursor (GPC) | NP: encapsidation of genomic RNA; GPC: cleaved into GP1 and GP2 for receptor binding and membrane fusion |
The L segment encodes the viral RNA-dependent RNA polymerase (RdRp or L protein), which is responsible for replication and transcription of the viral genome [1]. The S segment utilizes an ambisense coding strategy. It encodes the nucleoprotein (NP) in the negative-sense orientation and the glycoprotein precursor (GPC) in the positive-sense orientation [1]. The GPC is post-translationally cleaved by host cell proteases (e.g., SKI-1/S1P) into the mature glycoproteins GP1 and GP2, which form the trimeric spikes on the virion surface [1].
Viral Replication Cycle
The reptarenavirus replication cycle follows the general paradigm for arenaviruses, though specific details for snake hosts are still being elucidated.
Attachment and Entry: The viral glycoprotein GP1 binds to an unknown cellular receptor(s) on the surface of susceptible snake cells. Following receptor binding, the virus is internalized via receptor-mediated endocytosis. The acidic pH within the endosome triggers a conformational change in GP2, which mediates fusion between the viral envelope and the endosomal membrane, releasing the viral ribonucleoprotein (RNP) complex into the cytoplasm [1].
Replication and Transcription: The RNP complex, consisting of the viral RNA segments encapsidated by NP and associated with the L protein, serves as the template for both transcription and replication. The L protein first transcribes the viral mRNAs from the genomic RNA. For the S segment, this involves transcription of NP mRNA from the genomic template and GPC mRNA from the antigenomic template. Replication proceeds through the synthesis of full-length antigenomic intermediates, which then serve as templates for the production of new genomic RNA segments [1].
Assembly and Budding: Newly synthesized NP encapsidates progeny genomic RNA segments. The L protein is also incorporated into the RNP. These RNPs traffic to the plasma membrane, where the glycoproteins GP1 and GP2 are embedded. Virus assembly occurs at the plasma membrane, and progeny virions bud from the cell surface, acquiring their lipid envelope in the process [1].
Pathogenesis and Clinical Disease
Reptarenaviruses are the primary etiological agents of inclusion body disease (IBD) in snakes [1]. The hallmark of IBD is the accumulation of large, eosinophilic, intracytoplasmic inclusion bodies within cells of multiple organ systems, particularly the central nervous system, liver, kidney, pancreas, and oral mucosa. These inclusions are composed of aggregated viral nucleoprotein [1].
Clinical Signs: The clinical presentation of IBD is highly variable and depends on the snake species, viral strain, and route of infection. Common clinical signs include:
- Neurological Signs: Opisthotonos (stargazing), head tremors, incoordination (ataxia), disorientation, paresis, and paralysis. These are among the most characteristic signs of IBD [1].
- Behavioral Changes: Anorexia, lethargy, and regurgitation.
- Other Signs: Chronic respiratory infections, stomatitis, dermatitis, and secondary bacterial infections due to immunosuppression.
The disease is often progressive and fatal, particularly in bold snakes (boas and pythons). Some snakes, especially certain boa species, may remain subclinical carriers for extended periods, shedding virus intermittently and serving as a source of infection for other animals [1].
Host Range and Transmission
The primary hosts for reptarenaviruses are snakes of the families Boidae (boas) and Pythonidae (pythons) [1]. The virus has been identified in numerous species, including boa constrictors (Boa constrictor), annulated tree boas (Corallus annulatus), and various python species. Transmission is believed to occur through direct contact with infected snakes, their secretions (e.g., saliva, feces), or contaminated fomites. Vertical transmission (from parent to offspring) has also been suspected. The high prevalence of infection in captive collections suggests that the virus can spread efficiently under crowded or poorly managed conditions. For general care information on susceptible species, refer to the Corn Snake Care and Enclosure Setup guide, though it is important to note that IBD is more commonly reported in boids and pythons.
Diagnostic Approaches
A definitive diagnosis of reptarenavirus infection requires laboratory confirmation. Several diagnostic modalities are available.
Histopathology: Examination of tissue biopsies (e.g., liver, kidney, pancreas) or necropsy specimens for the presence of characteristic eosinophilic intracytoplasmic inclusion bodies. While suggestive, this method is not specific, as similar inclusions can be seen in other conditions. Immunohistochemistry (IHC) using antibodies against reptarenavirus NP can increase specificity [1].
Molecular Diagnostics (RT-PCR): Reverse transcription polymerase chain reaction (RT-PCR) is the gold standard for detecting reptarenavirus RNA. Assays targeting conserved regions of the L or S segment are highly sensitive and specific. Real-time RT-PCR (qRT-PCR) allows for quantification of viral load. Samples can include whole blood, plasma, swabs (oral, cloacal), or tissue biopsies. For a comparative analysis of molecular versus classical diagnostic methods, see PCR vs Virus Isolation in Veterinary Virology: A Comparative Analysis of Molecular and Classical Diagnostic Approaches.
Virus Isolation: The virus can be isolated from infected tissues or blood by co-cultivation with susceptible cell lines, such as the boa constrictor kidney cell line (BoaK) [1]. Isolation is time-consuming and requires specialized biosafety facilities, but it is essential for definitive characterization of new viral strains.
Serology: Enzyme-linked immunosorbent assays (ELISAs) and indirect immunofluorescence assays (IFAs) have been developed to detect antibodies against reptarenavirus NP. Serology can be useful for identifying previously exposed animals, but it may not distinguish between active infection and past exposure.
Diagnostic Decision Workflow:
flowchart TD
A[Snake with clinical signs suggestive of IBD], > B{Antemortem testing?}
B, Yes, > C[Collect whole blood & oral/cloacal swab]
C, > D[Perform qRT-PCR for Reptarenavirus]
D, Positive, > E[Confirmatory sequencing or virus isolation]
D, Negative, > F[Consider other differentials; retest if suspicion high]
B, No, > G[Postmortem examination]
G, > H[Collect tissues: liver, kidney, brain, pancreas]
H, > I[Histopathology & IHC for inclusion bodies]
I, Positive, > J[RT-PCR on tissue homogenate for confirmation]
I, Negative, > K[Consider other etiologies]
E, > L[Definitive diagnosis: Reptarenavirus positive]
J, > L
Management and Control
There is no specific antiviral treatment for reptarenavirus infection. Management focuses on supportive care, prevention of secondary infections, and strict biosecurity to prevent spread.
- Quarantine: New snakes should be quarantined for a minimum of 90 days and tested for reptarenavirus before introduction to an established collection.
- Biosecurity: Implement strict hygiene protocols, including the use of dedicated equipment for each animal or group, and disinfection of enclosures and fomites. Arenaviruses are enveloped and are generally susceptible to common disinfectants (e.g., bleach solutions, quaternary ammonium compounds).
- Culling: In many collections, euthanasia of confirmed positive animals is recommended to prevent further spread, especially in valuable breeding colonies.
- Supportive Care: Affected snakes may require fluid therapy, nutritional support, and treatment for secondary bacterial or parasitic infections.
Frequently Asked Questions
What is the primary cause of inclusion body disease (IBD) in snakes?
The primary cause of IBD is infection with viruses of the genus Reptarenavirus, family Arenaviridae [1].
How is reptarenavirus transmitted between snakes?
Transmission is thought to occur through direct contact with infected individuals, their bodily secretions, or contaminated fomites [1].
What are the most common clinical signs of IBD in snakes?
The most characteristic signs are neurological, including opisthotonos (stargazing), head tremors, ataxia, and paresis, often accompanied by anorexia and lethargy [1].
How is reptarenavirus infection definitively diagnosed?
Definitive diagnosis is achieved through detection of viral RNA via RT-PCR on blood, swabs, or tissue samples, or by virus isolation in cell culture [1].
Is there a treatment for reptarenavirus infection?
No specific antiviral treatment exists. Management is supportive and focuses on biosecurity and preventing further transmission [1].
Can healthy-looking snakes carry reptarenavirus?
Yes, subclinical carriers, particularly in some boa species, can shed the virus intermittently without showing clinical signs [1].
References
[1] Stenglein MD, Sanders C, Kistler AL, et al. Identification, characterization, and in vitro culture of highly divergent arenaviruses from boa constrictors and annulated tree boas: candidate etiological agents for snake inclusion body disease. mBio. 2012;3(4):e00180-12. URL: https://pubmed.ncbi.nlm.nih.gov/22893382/ *** Disclaimer: This article is for educational and informational purposes only. It is not intended to substitute for professional veterinary advice, diagnosis, treatment, or regulatory guidance. Always consult a licensed veterinarian or qualified specialist regarding animal health, disease diagnosis, and therapeutic decisions.